Q1. Is a BERA test painful or dangerous for young children?
No, the BERA test is completely non-invasive, safe, and entirely painless. It reads the natural electrical activity already generated by the nervous system. The surface electrodes stick to the skin like small stickers, and the sounds played through the earphones are set to safe, controlled volumes.
Q2. How long does a combined BERA and ASSR evaluation take?
A standard standalone BERA test takes between 30 to 45 minutes of quiet sleep time. If an ASSR evaluation is performed simultaneously or consecutively to build a detailed frequency map, the entire procedure generally takes between 60 to 90 minutes.
Q3. Can a BERA test detect an acoustic neuroma?
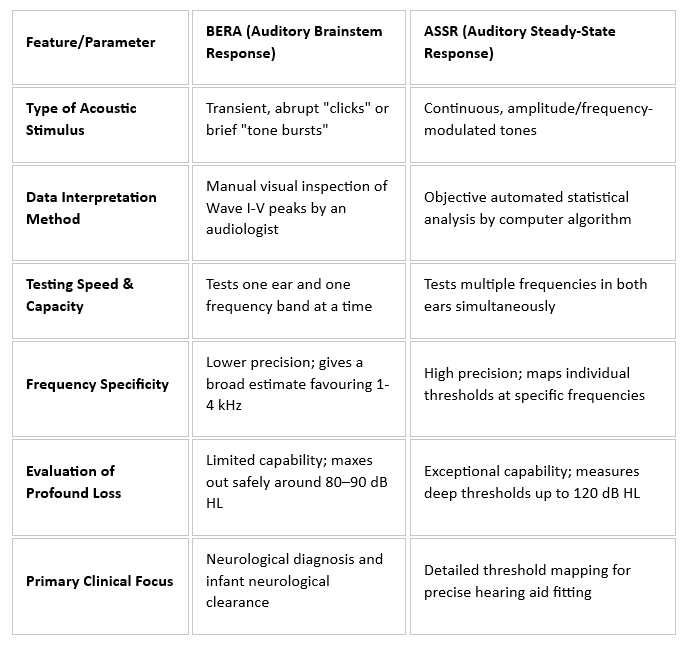
Yes. BERA is highly sensitive to changes in neural timing. If a benign tumour like an acoustic neuroma is pressing against the auditory nerve, it slows down the transmission of electrical signals, causing abnormal wave latencies (specifically delaying Wave V) when compared to the healthy ear.
Q4. Why choose ASSR over BERA if a child has profound hearing loss?
ASSR is preferred for profound hearing loss because it uses continuous modulated tones that can safely deliver higher sound intensities (up to 120 dB HL) than BERA’s brief clicks. This helps audiologists determine if the child has usable residual hearing or if a cochlear implant is the better option.
Q5. Can a BERA or ASSR test be performed while the patient is awake?
Adults can remain awake if they can sit completely still and keep their facial and neck muscles fully relaxed. For infants and young children, however, the test must be performed while they are asleep, as movement and muscle tension can obscure the delicate brainwaves being measured.
Q6. What is the difference between sensorineural and retro cochlear hearing loss?
Sensorineural hearing loss generally refers to damage located inside the inner ear’s hair cells (cochlea). Retro cochlear hearing loss refers to issues located further along the auditory pathway, such as the auditory nerve or the brainstem pathways that transmit those signals to the brain.
Q7. Does a flat line on a BERA wave chart mean a child is completely deaf?
Not necessarily. A flat line indicates that no synchronous neural response was detected at the test’s maximum output limits. It points to a severe-to-profound hearing loss, but an ASSR test or further clinical evaluation is needed to check for ultra-high frequency residual hearing or potential auditory neuropathy.
Q8. How should parents prepare an infant for an unsedated BERA test?
Parents should try to keep the infant awake and active for a few hours before the appointment and bring them to the clinic hungry. Feeding the infant right before the test begins inside the quiet room is an effective way to help them fall into the deep, natural sleep required for the evaluation.
Q9. Can middle ear fluid alter the results of a BERA or ASSR test?
Yes. If fluid is trapped in the middle ear (a condition called Otitis Media with Effusion), it acts as a physical barrier that softens the sound before it reaches the inner ear. This shifts wave latencies and raises thresholds, which is why a quick pressure test (tympanometry) is usually performed first.
Q10. Are the results of BERA and ASSR tests available immediately?
Yes, the raw data wave charts and statistical confirmations are generated in real-time by the testing computer. However, a paediatric or diagnostic audiologist must carefully review, interpret, and cross-reference these findings to construct a formal, actionable diagnostic report.